
The litigious patient
There is a four-fold greater chance of litigation for any medical or dental practitioner in the UK compared with a practitioner in New York
Make no mistake, we’re no longer mimicking the US culture of litigation – we’re now leading the world. So, whether you’re a dentist, a doctor, or in the business of offering legal representation to either, it’s well worth understanding just who’s driving this financially and emotionally expensive cultural revolution. Is there a particular species of litigious patient, and if so, what do they look like?
The answer is obviously ‘no’, but there are certainly patterns of behaviour and traits of character that have become apparent to me during more than 30 years as a restorative dentist, and as an expert witness with experience of both sides of the judicial fence. Of course, it’s preferable to avoid any patient-practitioner relationship developing into full-blown litigation in the first place. Complaints invariably originate from poor communication, and can be provoked by what is said, is not said, or both.
My own audit of more than 20 years of documentation revealed the following triggers that led to the patients issuing civil proceedings, in descending order of frequency:
1. A sense of abandonment and failure to respond when problems became apparent.
2. Miscommunication with an English-speaking patient due to the clinician’s mother tongue not being English.
3. Failure to identify that the clinician is out of his/her depth and a referral to a colleague clearly indicated.
4. The absence of the usual clinician due to illness or holiday, causing the patient to attend another practitioner who makes a negative comment about their dental state, eg untreated periodontal disease or tooth decay.
5. Failure to adhere to well-established clinical protocols, with specific reference to alternative therapies with no scientific or clinical data to support their use.
6. Early failure of the treatment with unsuccessful efforts to resolve the problems.
7. A report that the clinician was too brusque and/or rude and appeared in a hurry.
8. Patients reporting that the clinician lost his cool/patience and/or shouted at them.
It often transpires that the ‘offending’ practitioner has chivvied a patient into making a choice using demanding or dictatorial language, whether real or perceived. A recent review of complaints carried out by one of the leading dental defence indemnity insurers concluded that more than 70 per cent of complaints were attributed to poor communication, highlighting not only indelicate vocabulary but the manner of delivery and body language, suggesting a lack of ‘feeling’ or compassion.
In contrast – and in a great many of the cases I’ve encountered – clinicians attempt to abandon the patient by not responding to letters of complaint and not returning phone calls. An apology, accompanied by some shared expression of concern and regret, plus an assurance that the problem will be rectified, is often all that’s needed to prevent the matter escalating and the patient taking their grievance to a third party.
Unfortunately, with the best will in the world, clear communication sometimes isn’t enough and the motive of revenge or financial gain can mean a practitioner’s reasonable defence falls on deaf ears. When financial compensation is an unlikely outcome, I’ve observed that writing to governing authorities can become the means by which some patients aim to ‘get back’ at the clinician, ‘teaching them a lesson’ and ‘protecting others from harm’.
I’m confident that patients particularly prone to this course of action have an identifiable character profile. Patientes Litigiosum is almost inevitably female and over 50 years of age. Before I’m accused of sexism, my own audit revealed that 90 per cent of our own claimants – those bringing formal suits against my own clinic – were female. This can be explained by the higher percentage of female patients with long-standing prosthodontic issues referred to the clinic. But a review of all our medico-legal referrals to me as an expert witness and involving litigation suits against general dental practitioners over the last three years revealed a 60 per cent female bias.
Figure 1
Issues considered by the GDC’s PCC/PPC in 2015
| ISSUE | NUMBER OF OCCURRENCES** | % OF TOTAL OCCURRENCES |
|---|---|---|
| Poor treatment | 179 | 23% |
| Poor record keeping | 111 | 14% |
| Failure to take appropriate radiographs or to interpret | 80 | 10% |
| Fraud/dishonesty | 53 | 7% |
| Failure to obtain consent/ explain treatment | 42 | 5% |
| Failure to cooperate with the GDC or failure to disclose convictions/cautions | 38 | 5% |
| Personal behaviour | 33 | 4% |
| Prescribing issues | 31 | 4% |
| Working outside scope of practice | 25 | 3% |
| No professional indemnity insurance of failing to produce evidence | 24 | 3% |
| Undiagnosed/untreated caries | 21 | 3% |
| Cross-infection control | 16 | 2% |
| Failings in recording medical and/or dental history | 15 | 2% |
| Conviction or caution – other | 14 | 2% |
| Misleading advertising | 11 | 2% |
| Conviction or caution – assault | 10 | 2% |
| Indecent assault or inappropriate sexual behaviour | 10 | 1% |
| Misled about treatment available on the NHS | 9 | 1% |
| Conviction or caution – alcohol or drugs | 9 | 1% |
| Conviction or caution – theft/robbery | 8 | 1% |
| Failure to refer | 7 | <1% |
| Period of unregistered practice | 5 | <1% |
| Clinically incorrect extractions | 4 | <1% |
| Failure to anaesthetise | 4 | <1% |
| Failure to spot or monitor lesions | 3 | <1% |
| Failure to inform patient of adverse incident | 3 | <1% |
| Employing dentist or nurse not registered with GDC | 3 | <1% |
| Inaccurate statements to CQC | 3 | <1% |
| Tooth whitening | 2 | <1% |
| Making racially offensive comments | 1 | <1% |
| Not supervising Vocational Dental Practitioners adequately | 1 | <1% |
| Total | 775 | |
** Cases often involve more than one issue. These figures provide a profile reflecting the main issues involved, and not every single charge
Our litigant is invariably living alone or estranged from partner or family. If married, their relationships have become unloving and burnt out. It is highly likely they are possessed of a long mental health history of chronic anxiety and depressant illness previously treated with medication and/or cognitive behavioural therapy. Expect a high display of feelings when questioned during a consultation appointment. One will also observe multiple functional disorders, including gynaecological complaints, chronic fatigue syndrome, irritable bowel syndrome, and other ailments that long-suffering GPs have failed to ‘put their finger on’. Multiple visits to the GP for exhaustion and irregular sleep patterns are common. The problem for the busy clinician who, understandably, tends to focus on his/ her anatomical area of interest, can easily miss these traits. After all, the dentist is concentrating on the teeth, whereas the orthopaedic surgeon is in ‘bone mode’.
The traditional Western medical approach is collectively disease-focused, whereas the old Greek physician’s philosophy of focusing on “don’t tell me about the disease in the man, but about the man with the disease” could not be closer to the truth. An interview technique that subtly explores the personal, social and professional history is essential in gathering information necessary to the spotting of this high-risk group. Once identified, it then becomes a matter of explaining the interaction of stress and depression upon the immunological competences of a patient, and their ability to cope and heal following stressful surgical assaults. It allows you to share with the patient the responsibility of healing and get them ‘on board’. I have learnt that if a patient can readily connect the dots between their mental and physical health then all is well. However, if the patient vigorously denies any connection between the two, despite it being already abundantly clear, then I consider they’re assuming no responsibility and now refer the patient elsewhere. However, I always pass on this vital piece of information to the referred clinician. Fair’s fair.
-
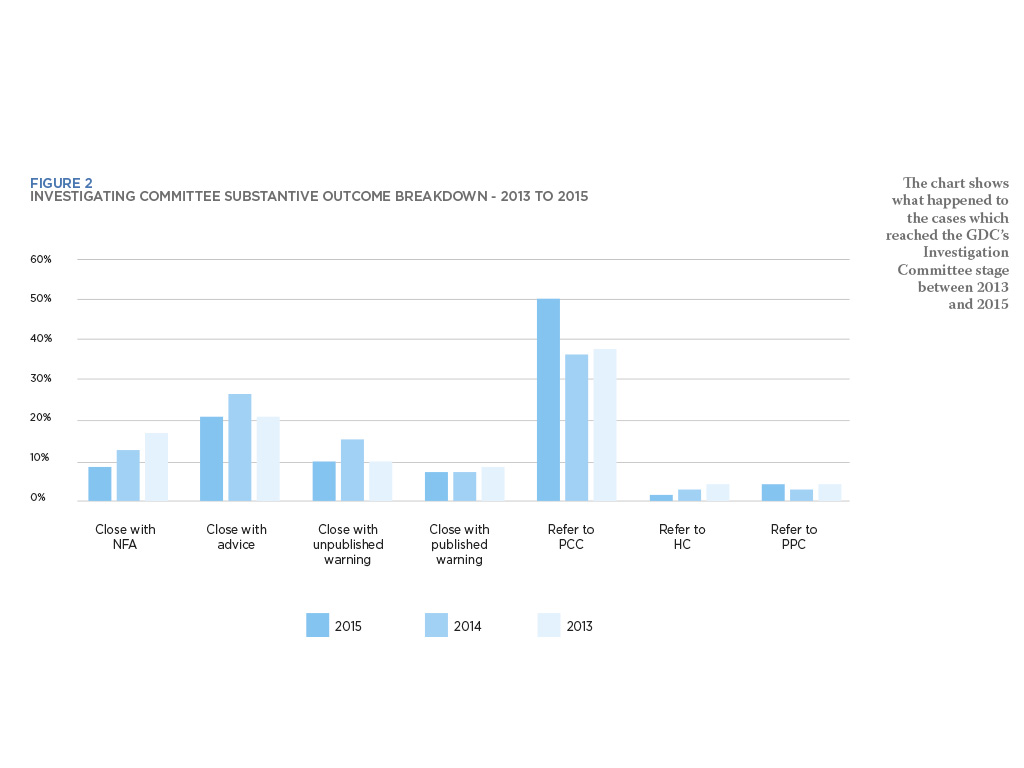
- Figure 2
-

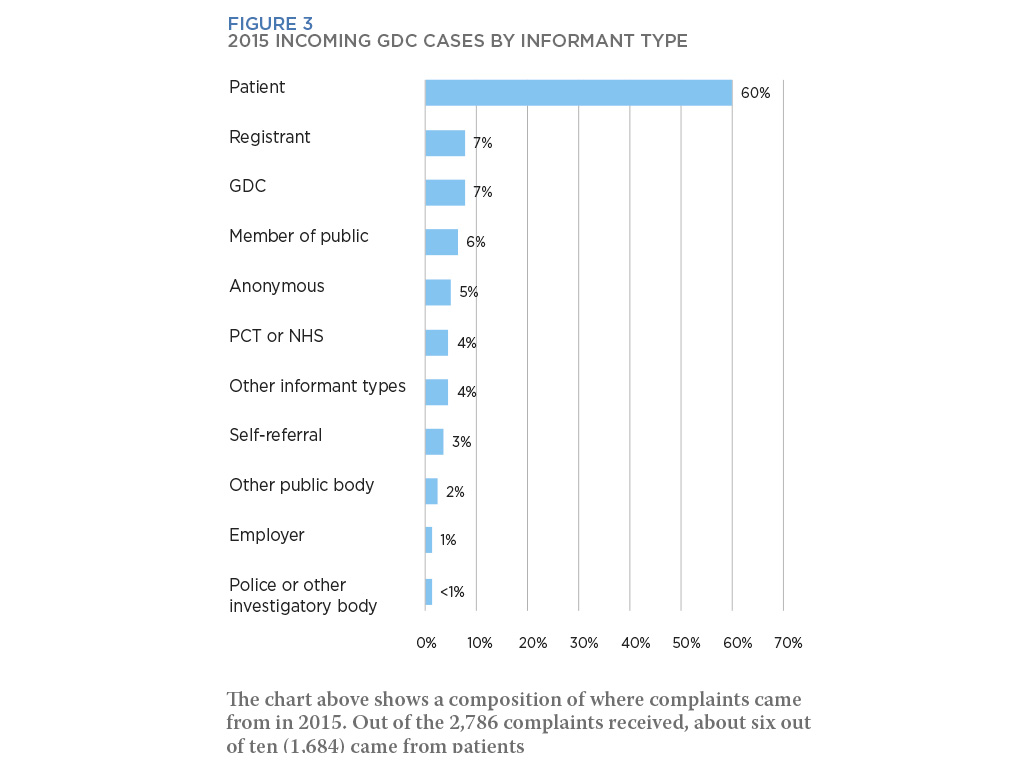
- Figure 3
The logic behind this approach is that I’ve now readily accepted that I cannot possibly connect with all patients all of the time. Where I might fail, another clinician may succeed. By way of an example, a Welsh patient required treatment that she was finding intolerant, and returned repeatedly with bizarre functional symptomology including atypical facial pains and additional locomotor skill loss. A referral to a Welsh consultant did the trick. He carried out a series of placebo adjustments and she reported an extraordinary resolution.
In my opinion, an Englishman was prejudiced from the start, despite the quality of care provided. Incidentally, she had a long history of depressive illness. A useful tool, sadly out of print since 1995 but which I continue to use, is the Cornell Medical Index Questionnaire. This will allow a clinician with no formal training in psychology or psychiatric medicine to identify these patients who often present with multisystem functional disorders.
Having identified the patient traits and context most likely to result in litigation, it seems only fair to consider whether there might be a similar species within the genus Medicus. Is it possible to be more or less prone to action as a practitioner? Although this is wholly anecdotal, I believe that clinicians with OCD characteristics and a liberal sprinkling of Asperger’s make excellent and highly-focused surgeons. But they’re prone to a greater number of complaints when compared with ‘touchy-feely’ clinicians.
Personally, I’d much rather have the indifferent, socially inept OCD character operating on my person than the ‘schmoozer’ who’s more readily distracted by peripheral events. Sadly, as new management practices in the medical arena now demand a more emotional ‘chairside’ manner from our doctors, dentists and surgeons, the public is unaware of what they’re losing. And here’s the rub – for the large part, the rise of the litigious patient helps no-one. The medical profession can maintain the highest possible standards of patient care, but it’s society as a whole that holds blame and scrutiny in balance.
About the author
Toby Talbot is clinical director at the Talbot Clinic. Over the last 17 years, he has established a professional fast-track service for the legal community, helping courts, counsel and judges make accurate and well-informed decisions.
Verifiable CPD Questions
Aims and objectives
• To catalogue the most common causes for litigious action against dentists
• To identify common behaviours in dental patients most prone to making litigious complaints
• To identify personality traits shared by litigious patients
• To consider the type of dentist most likely to attract litigious complaints.
Learning outcomes
• Good communication is essential to healthy dentist-patient relationships, especially following a complaint
• Failure to respond to patient dissatisfaction can be catastrophic
• In many cases a complaint or litigious action is an emotional response to longer term and wider-ranging mental and/or physical health issues
• Stress and depression can affect dental health and the efficacy and recovery from treatment.
Comments are closed here.