
Creating H.O.P.E. from challenge
Collaboration between a dental school and designers has led to a low-cost 3D-printed device allowing students to practise key skills remotely or, socially-distanced, in class
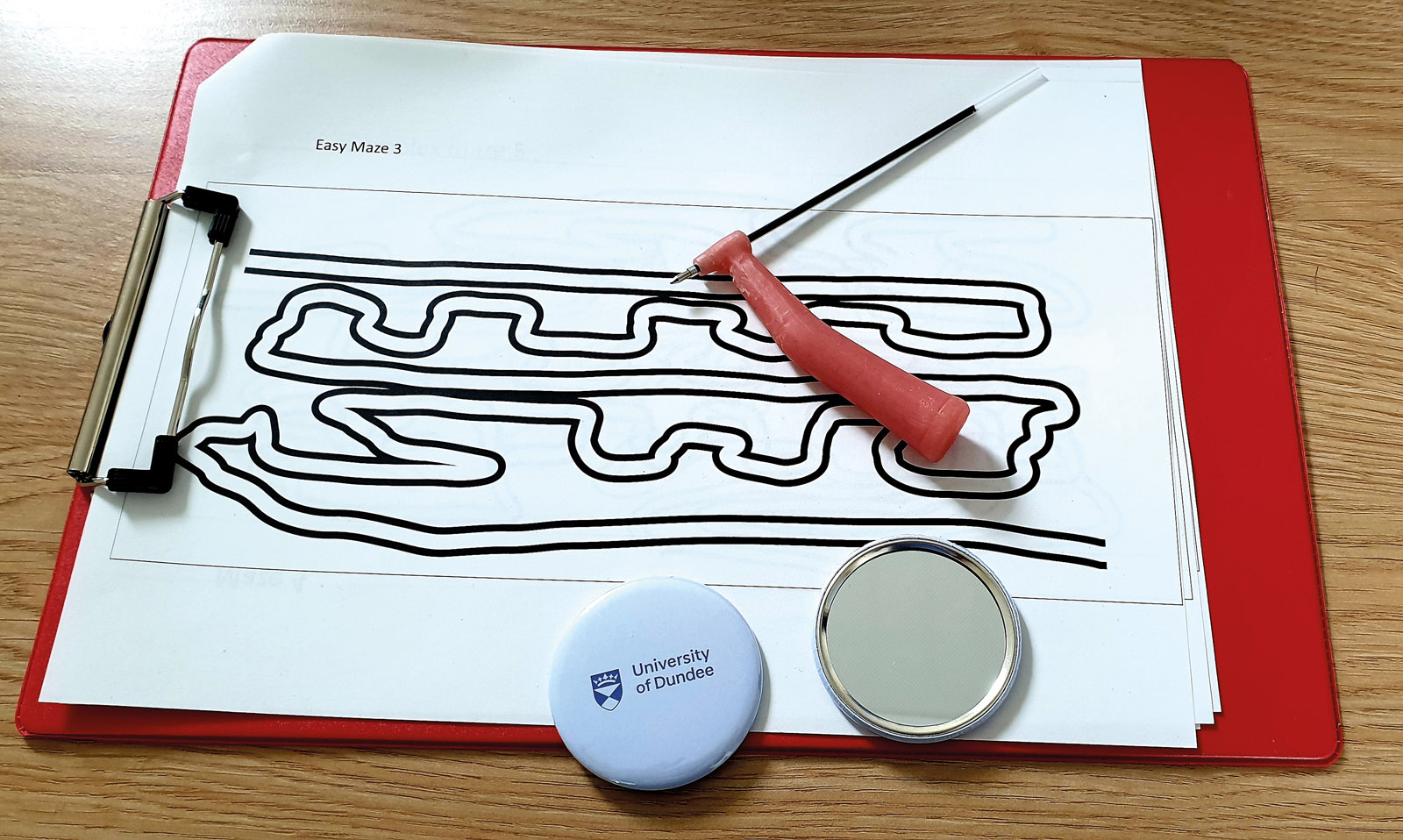
Figure 1 - The initial equipment set up used for the early skills development exercises
Two thousand and twenty was certainly a trying year for our profession. Virtually all aspects of dentistry encountered unique challenges as we approached uncharted territory; lockdowns, social distancing, aerosol generating procedures and furlough. At times, we think it is safe to say we all felt much the same as that first day at dental school, a heady mix of uncertainty and a drive to ultimately become immersed in patient care.
Married to a General Dental Practitioner, and my own work as a clinical lecturer in dentistry, it became apparent to me how varied were the challenges we all faced. However, the solutions to these challenges all had a common theme: innovation.
Problematic as 2020 proved to be, it could also be viewed as a catalyst for change. I stress catalyst rather than instigator. Dentistry, both in training and practice has always been an adaptive profession, striving to improve. The events of the past year merely accelerated and guided change.
I have witnessed countless examples of innovative solutions implemented by colleagues for dental training over the past year as universities have shifted towards a blended online and practical approach. It is unsurprising, given the dedication we all have to the profession, but nonetheless impressive.
I will detail here the development of H.O.P.E. – Home Operational Practice Equipment (if you have a good acronym, you are halfway there). This is a device that has the potential to allow students to practice key skills from home or remotely for a minimal cost. The development of this was accelerated throughout 2020 and it proved to be quite useful in meeting some of the unique challenges we encountered.
The problem
I have been interested in the integration of remote teaching and the early development of skills applicable to a broad range of dental procedures. Students learn skills at their own pace; as a student, I witnessed first-hand that a ‘one size fits all’ curriculum did not always work well. Students experienced genuine anxiety when they took a little longer than their colleagues to develop a clinical skill such as undertaking a composite restoration, perfecting the form and function.
Developing skills in a safe environment is key for dental training. However, with limited simulated training resources, students don’t always get the time they need to practice and develop their skills.
These problems have been exacerbated in the past year. Capacity of training spaces has been greatly reduced to accommodate social distancing guidelines, with the inevitable consequence of students having reduced hands-on experience.
The opportunities to practice and ‘self-discover’ have also been negatively affected. Additionally, as teaching moves to more online formats, there is less opportunity for impromptu informal discussions between the trainees and trainers.
All this before we even consider the reduced clinical experience.
Sparking a novel approach
I was fortunate to have been teaching during the transition at Dundee Dental School to the new 4D Curriculum. I had the opportunity to work on the development of a new early rotary instrument clinical skills course. This course was designed using modern educational principles, and executed with less conventional exercises, some of which required the creation of new equipment.
It was in 2018 that the initial concept of instrument analogues was implemented. The first iteration was a pen that simulated the angulations of a handpiece to instil the basic principles of instrument ergonomics in early year students. This was fabricated using expired denture acrylic in a silicone mould (Figure 1).

Using a mirror for indirect vision, students would use these pens to navigate mazes created by my colleague, Roddy Milne. Although the course was positively received, production times and cost were an issue. There was also the limitation of working on a flat surface rather than matching dental arch contours.
There were really two serendipitous events that occurred in the development of our equipment. Later that year, the University of Dundee opened a new Creative Space within the main library, where staff and students could work with several crafts, including 3D modelling and printing. Here I met Richard Parsons, CIO Director of the Library Learning Centre.
We discussed the overall concept and together explored CADCAM for streamlining the equipment and creating a prototype that could be printed. This had a number of advantages over simply creating moulds. We were able to create a design that could be modular and adaptive, with an internal screw thread (Figures 2 and 3).


Figure 3 – The Printed version of the pen being used with our revised exercise sheet
The second event that really accelerated this project would be the first nationwide lockdown due to the COVID-19 pandemic. Thus, several factors combined to create the perfect environment for collaboration and creation: a silver lining in the midst of some rather dark clouds.
How it developed
With the stay-at-home order in effect, the idea of a cheap alternative to a phantom head that could be used by students at home or isolating seemed more relevant than ever. I collaborated with a former dental student, Yu En Cheah, to convert my concept drawing into an initial 3D prototype. I had worked with Yu En on several teaching resources when he was an undergraduate and had every confidence in his resourcefulness.
We quickly created an initial prototype file and (Figure 4) printed for testing (Figure 5). It was around this time that we started collaborating with Alasdair Napier, a colleague at the renowned Duncan of Jordanstone College of Art and Design at the University of Dundee. For the past year, he has provided invaluable advice regarding 3D modelling development and committed printing resources towards the production of rapid prototypes, and ultimately the final product.

Figure 4 – Initial concept for baseplate with features to accommodate Indirect vision and positioning exercises

Figure 5 – Initial print out of device. This was a single component print, with limited application.
However, the most surprising collaboration, that lead to the final product, was with our current undergraduate students. We must always remember that our students come to the course with unique talents and an eagerness to shape their education. They also have the most contemporaneous insight into their training needs.
Tung Hin Lau and Desmond Manangazira had some experience in creating and printing 3D models. I was amazed at how quickly they adapted and developed these skills for this project. Tung was working at home from an apartment in Hong Kong at this uncertain time, with limited access to computer resources. Even with these constraints, he was able to produce incredible designs within short time frames. Their dedication and commitment, to say the least, continues to impress me.
It was important that we made our goals realistic. The functionality of any training activity, undertaken outwith a clinical skills laboratory, cannot require suction, rotary instruments and pressurised air or water. Furthermore, safety considerations regarding potentially unsupervised activities must be considered; particulate generating and cutting exercises were not practically viable as these would require close supervision and access to costly equipment and air compressors and high-volume suction.
We decided to focus on three key concepts that would provide good foundation for early year dental students:
- Restoration of dental arches and tooth anatomy;
- Rotary instrument ergonomics;
- Operating with indirect vision.
The key principle for this was modularity. This allowed us to facilitate any custom attachments, provided they fit the connector. This would also allow for more exercises to be carried out on a universal baseplate, reducing the materials needed for production and saving on space.
Design of base plates for the maxilla and mandible were first sketched out from imagination. These were then re-imagined as 3D objects, utilising software programmes including Rhino, Fusion 360 and Meshmixer. We completed multiple revisions until the desired form was created. Key considerations included:
- Technical limitations;
- Environmental impact;
- Practical application;
- Future implementation;
- Cost and time to print.
3D printing technology, though revolutionary, has some key limitations that needed to be factored in at the design stage. One of the main factors when considering the design was the limitation of using flatbed printers in the production of models with undercuts. All components needed to be designed to cater for the tolerances that our available printers had for predictably and reliably producing undercut angles. There are many different types of printers and having a detailed knowledge of those available is crucial.
It became apparent that it would not be possible to print the base model as one unit. The universal connector needed to be printable with the facilities available and suitable for use by students without training. Drawing on classic joinery techniques, used for years in carpentry, we planned all connectors and joints with clear paths of insertion, while also maximising rigidity and retention.
The final streamlined design was formed with angles, simulating the degree at which the mouth would be positioned with a patient semi-recumbent in the dental chair. Tolerances were calculated so that no overhangs would be produced, and the overall shape would print out without the need of support material.
Prototypes of the entire device, as well as specific component joints, were printed and tested for ease and reliability of use. To allow a margin of freedom, spaces had to be made for easier movement and less resistance between female and male joints in the device linking base connectors and modular components.
Exercise components were created by stitching models together in Cura, another software programme, allowing print quality to be retained for exercises that required detail. This created the potential for incorporating 3D scans of dentitions into our models.
Other areas of consideration when designing this model were the limitations and strengths of the printable materials available. Different materials such as polylactic acid (PLA) or Acrylonitrile Butadiene Styrene (ABS) plastic had different 3D printing properties. Some had better properties for reproducing fine detail, yet possibly lacked the strength required for a connector joint. Over and above this, we needed to choose materials that were able to be decontaminated in accordance with changing guidelines.
As a result of all these collaborations, we have now produced a base model set that can easily be adapted for various functions (Figures 6 and 7).

Figure 6 – Our current model: Here we can see that this is made of several
interlocking components. The modular design allows for
numerous attachments

Figure 7 – An example of a student working from home undertaking a tooth carving exercise
Where we are now
We had a fully functional model by October 2020 and printed a limited run of 22 units. Although the initial plan was to produce designs for a home kit, these devices have now been used in a variety of practical classes within the Dundee Dental School. Eighteen of the units were set up in a lecture theatre that now lacked the space for social distancing to serve in its original function (Figure 8).

Figure 8 – An example of how a lecture theatre has been repurposed as a hands-on skills training space
This allowed us to teach classes outside of our clinical skills laboratory, increasing student ‘hands-on’ training, as well as reducing the pressure on the valuable, yet limited teaching space. Classes were run for both second- and fourth-year students. The second years reconstructed teeth using modelling clay and practiced the application of fissure sealants. Additional attachments were made to facilitate a fourth-year undergraduate orthodontic clinical skills course, which was run entirely in our repurposed teaching space (Figure 9).

Figure 9 – The unit set up for undertaking an orthodontic training course
Another application of this equipment became apparent as the year progressed. In the previous issue of Scottish Dental magazine, our colleague Professor Grant McIntyre detailed how he won an incredible battle with COVID-19. On leaving hospital, Grant was keen to strengthen his skills and return to work as soon as possible.
This is obviously a very different situation to that of the novice student. We were able to rapidly combine complicated malocclusion scans with our connectors to allow for custom exercises. A kit was produced and delivered (Figure 10). Shortly thereafter, we received very positive feedback from Grant, giving us a truly unique insight into another potential use of H.O.P.E. for clinicians looking to regain practical skills after a long break from the profession.

Figure 10 – Example of a take-home kit, demonstrating how easy it is to customise for bespoke exercises
The road ahead
The potential for all this is quite exciting. By focusing on creating the 3D printable STL files, units can be produced anywhere with access to printers. The cost per complete unit with models for various exercises is minimal, at around £30 for the set. Individual exercise modules can be produced for about £2 each.
We have the potential to collaborate internationally. It is reasonably straightforward for dentists with CADCAM skills to produce custom attachments. Our colleague, Richard Boyle, demonstrated this by developing a set of models with teeth missing for our students to ‘restore’. Our overarching principle is collaboration for the benefit of our future colleagues. It would be entirely possible to create an STL repository with a myriad of custom exercise modules.
We are still developing designs and looking into potential applications. I am intending to undertake research to validate its efficacy as an educational tool. The times are calling for change in how we approach training and education. Synergistic collaborations with other disciplines have great potential to yield exciting outcomes. This project would not have been possible without the support we had both from the Dental School and from the wider university. We must embrace all the tools at our disposal and look at these changes as potential enhancements rather than substitutions.
Comments are closed here.