Getting personal with the dental check-up: are risk-based recalls risky?
How often to recall our patients is perhaps the most common decision dentists make. Traditionally most adult patients are used to having a check-up every six months, regardless of an individual’s risk of oral disease. The most recent Adult Dental Health Survey reported that 61 per cent of dentate adults said the usual reason they attend the dentist is for a regular check-up1. The dental check-up can be considered to have a dual function in primary and secondary prevention. Early signs and symptoms of oral disease can be detected, in particular dental caries and periodontal disease, as well as a systematic examination of the oral mucosa2–5. Preventive advice can also be provided where appropriate and may incorporate oral hygiene instruction, dietary advice, and smoking cessation or alcohol-related health advice if appropriate6,7.
Extending intervals between dental check-ups from six months to 18 months was proposed by Aubrey Sheiham in 1977 who concluded: “No evidence was found to support six-monthly dental checks” 8. Recall intervals between check-ups based on patient risk assessment have been endorsed by professional expert bodies, dental health service reform initiatives and clinical practice guidelines in several countries9–11. The 2004 National Institute for Health and Care Excellence (NICE) guidance recommends that the interval between check-ups “should be determined specifically for each patient and tailored to meet his or her needs, on the basis of an assessment of disease levels and risk of or from dental disease”12. Based on the NICE guidance the Scottish Dental Clinical Effectiveness Programme (SDCEP) published their Oral Health Assessment and Review guidance in 201113. However, until now the evidence to support these recommendations was of low-quality.
October 2020 saw the publication of an updated Cochrane review Recall intervals for oral health in primary care patients14; its aim to identify the best time interval between dental check-ups. The review included randomised controlled trials conducted in general dental practices and is, therefore, of direct relevance to this setting. This review found two clinical trials investigating the effect of different check-up frequencies – including one recently completed trial – the INTERVAL Dental Recalls Trial15. This trial assessed patients attending the dentist either every six months, every 24 months, or attending for a check-up based on their likely risk of disease on a personalised risk-based recall interval. Recruiting dentists considered if each individual was suitable to be seen on a 24-month recall interval prior to random allocation to a recall strategy. Those patients where a 24-month interval was considered appropriate were randomised to one of three groups – six-monthly, 24-monthly or risk-based recall. Those patients where a 24-month recall was not considered appropriate were randomised to either a six-monthly or risk-based recall. The clinical effectiveness and cost-effectiveness of these different recall strategies were assessed after a four year follow-up period across a broad range of clinical and patient-reported outcome measures: gingival bleeding on probing, periodontal disease, dental caries, calculus, patient well-being and patient satisfaction with treatment. Of the 51 dental practices and 2,372 recruited patient participants, 24 dental practices and 1,188 participants were from Scotland.
Consequently, the Cochrane review concluded that “there is high-certainty evidence that there is little to no difference in oral health outcomes when comparing six-month recall interval with a risk-based recall interval. In addition, there is moderate to high-certainty evidence that there is little to no difference in oral health outcomes when comparing a 24-month recall interval with either six-month or risk-based intervals”. The comparison with the 24-month recall interval reinforces the value of the risk-based interval as all participants on a 24-month recall had been risk assessed and considered eligible for this interval. The results of this review question whether a universal six-month check-up is the best frequency for check-ups when those attending based on risk or those low risk patients attending every two years had similar oral health after four years. The results also provide a positive message that dentists can accurately assess patients’ risk of oral health problems and allocate an appropriate recall interval based on this risk assessment.
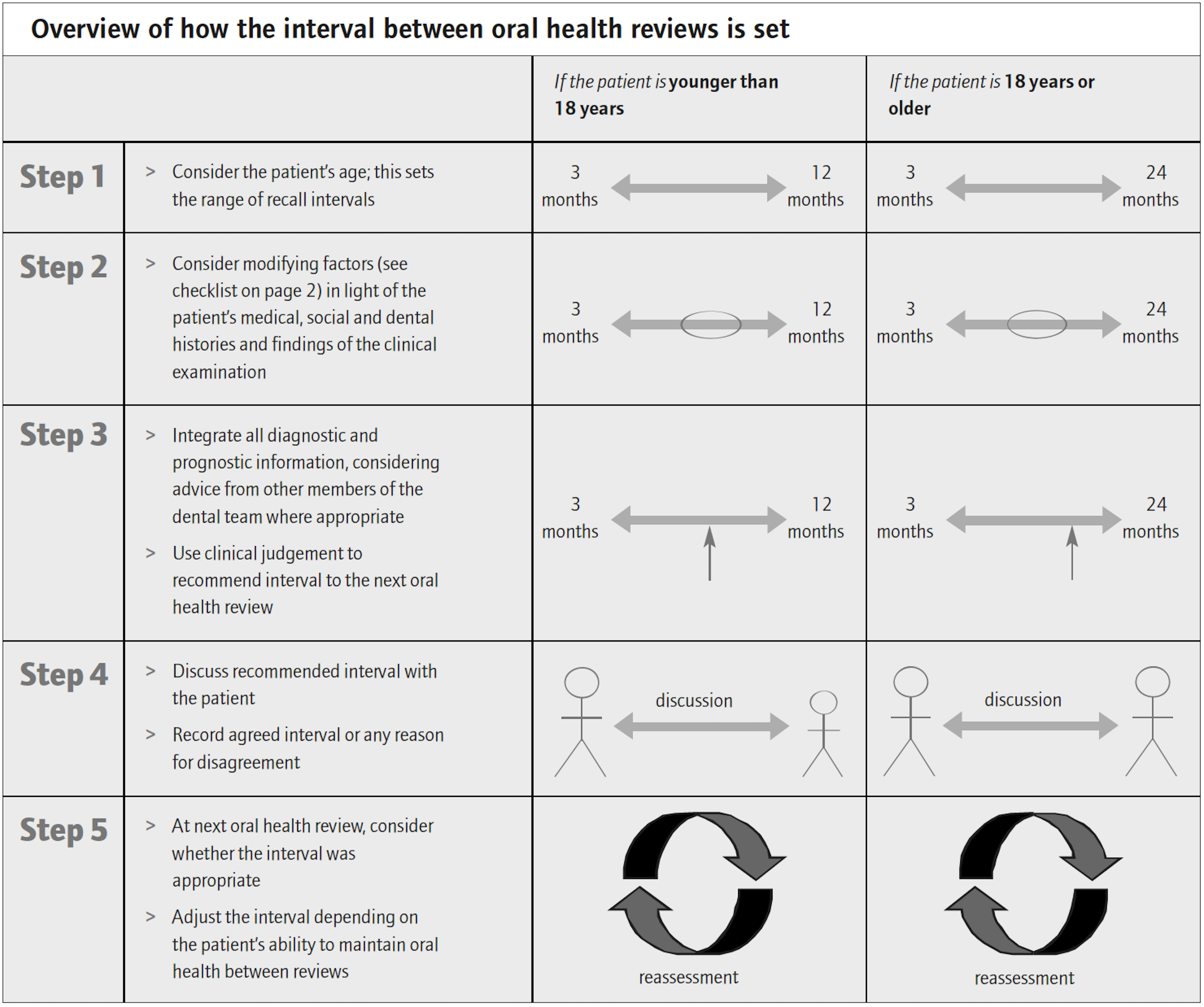
NICE guidance recommends a recall interval based on an assessment of an individual’s risk of dental disease, varying between three months to two years between check-ups in adults, reserving the longest interval for patients “who have repeatedly demonstrated that they can maintain oral health”12. The guidance recommends the longest interval of 12 months between check-ups in those younger than 18 years old. The guidance also outlines the various steps dentists can take to decide on an appropriate recall interval and is summarised in Figure 1.
Details on oral hygiene habits and timing, dietary habits – including amount and frequency of sugar intake, fluoride use, and tobacco and alcohol intake can be collected in a comprehensive history. A medical history can be assessed to identify factors that may impact on oral health. Further important information is assimilated from a thorough clinical examination, where signs of active disease can be identified, plaque control and potential retentive factors evaluated, and quantity and quality of saliva assessed. Past disease experience can also be assessed through the number of restored and missing teeth. This can be a difficult component to integrate into the risk profile of new or recent patients where uncertainty around the timing of restorations or extractions remains following history and examination. A number of supporting tools have been developed and supplied with the SDCEP guidance to assist practitioners in the collection of appropriate information to aid risk assessment13.
Integration of this collected information allows the clinician to use their clinical judgement to predict the individual’s likely future disease experience and recommend an appropriate tailored recall interval based on this risk assessment. This is a joint decision between clinician and patient and involves discussing the recommended interval, exploring patient preferences and expectations, and discussing any relevant financial implications. An agreed interval should result and be recorded along with a record of patient views, particularly useful where these may differ from the clinician. In circumstances where uncertainty regarding an individual’s disease risk occurs, an initial conservative recall can be extended where maintenance of oral health is demonstrated over time.
Consideration of the appropriateness of the previous recall interval in terms of health outcomes and patient views can inform clinician and patient joint decision making on the next interval between dental check-ups. The interval may be maintained at the same level if it is achieving its aims. Where disease activity is low, the recall interval can be gradually extended towards the 24-month maximum period. Where disease activity progresses, a shorter recall interval and more intensive preventive care may be considered. Individual risk factors and therefore risk of dental disease change over time. Where exposure to new risk factors are identified at dental recall appointments, previously longer recall intervals can be adjusted to account for changes in likely future disease experience. Clinicians should continue to use dental recall appointments to provide advice on reducing the patient’s risk factors and enhance protective factors.
Dentist confidence in their perceived ability to assess risk increased with their experience of conducting risk assessments over the four-year trial period. With experience, clinicians should be able to carry out a risk assessment quickly and intuitively as part of each recall appointment.
One of the persistent arguments in favour of maintaining six-monthly dental check-ups is that dentists may miss the opportunity to diagnose oral cancer lesions at an early stage in patients who attend at longer recall intervals. The incidence of oral cancer in the UK is highest in Scotland, at 10.0 per 100,000 males16. However, it has been reported that 53.7 per cent of patients diagnosed with oral cancer had not attended a dental check-up at all in the two years preceding diagnosis17. It is estimated that dentists in Scotland will see a case of oral cancer once every 10-20 years17 – depending on the geographical location.
In addition, risk factors for oral cancer are similar to risk factors for dental caries and periodontal disease – smoking and alcohol intake and individuals from lower socioeconomic status are at increased risk of all three diseases. A personalised risk-based recall would therefore allow those individuals at greater risk to be seen more frequently while healthy patients can be seen less frequently. The UK National Screening Committee advises the NHS about screening programmes for all diseases and has considered oral cancer screening rejecting it on several occasions18. Examination of the oral mucosa is still recommended at every recall, as is the recall of patients at high risk of dental disease and oral cancer more frequently than patients at low risk of these diseases.
A recent article in The Lancet commented on the opportunity afforded to dental services by the COVID-19 pandemic19 – specifically re-orientation towards a less invasive and more preventive approach, prioritising care for high need groups and ceasing ineffective treatments that do not improve health outcomes. Considering that the NHS in Scotland delivered 2.8 million dental check-ups in 2018-19, accounting for 15 per cent of all primary care dental spending20, there would appear to be opportunities for cooperation between health care policy makers, clinicians and patients to ensure patients are receiving treatment supported by contemporary scientific evidence.
The results of this research are particularly valuable when considering the impact of the COVID-19 pandemic – dental practices have been closed, patient access for dental treatment has been limited, and access to dental care may remain limited for some time. But the results of this review provide reassurance to those seeking and providing dental treatment, that intervals between check-ups can be extended beyond six months without detriment to oral health. The enforced extended time between dental visits may also provide an opportunity for practitioners to identify patients at higher or lower risk of oral disease.
Risk factor variables from the NICE dental recall checklist
Medical history
Social history
Dietary habits
Exposure to fluoride
Clinical evidence and dental history
- Recent and previous caries experience
- Recent and previous periodontal disease
- Mucosal lesion
- Plaque
- Saliva
- Erosion and tooth surface loss
‘Overview of how the interval between oral health reviews is set’ © NICE 2004 Dental Recall – Recall interval between routine dental examinations. Available https://www.nice.org.uk/guidance/cg19/evidence/full-guideline-appendices-f-g-pdf-193348913. All rights reserved. Subject to Notice of rights. Reproduced by kind permission from the National Institute for Health and Care Excellence (NICE). NICE guidance is prepared for the National Health Service in England. All NICE guidance is subject to regular review and may be updated or withdrawn. NICE accepts no responsibility for the use of its content in this product/publication.
References
1 Hill KB, Chadwick BL, Freeman R, O’Sullivan I, Murray JJ. Adult Dental Health Survey 2009: Relationships between dental attendance patterns, oral health behaviour and the current barriers to dental care. Br Dent J 2013; 214: 25–32.
2 British Dental Association. Opportunistic Oral Cancer Screening. BDA Occasional Paper. London: British Dental Association, 2000. .
3 Clovis J, Horowitz A, Poel D. Oral and pharyngeal cancer: practices and opinions of dentists in British Columbia and Nova Scotia. J Can Dent Assoc (Tor) 2002; 68: 421–5.
4 Conway DI, Macpherson LMD, Gibson J, Binnie VI. Oral cancer: prevention and detection in primary dental healthcare. Prim Dent Care 2002. doi:10.1308/135576102322481938.
5 Field EA, Morrison T, Darling AE, Parr TA, Zakrzewska JM. Oral mucosal screening as an integral part of routine dental care. Br Dent J 1995. doi:10.1038/sj.bdj.4808894.
6 National Institute for Health and Care Excellence. Oral Health Promotion: General Dental Practice. 2015. Available from www.nice.org.uk/guidance/ng30. .
7 Public Health England. Delivering Better Oral Health: an Evidence-based Toolkit for Prevention 3rd edition. Available from assets.publishing.service.gov.uk/government/ uploads/system/uploads/attachment_data/file/605266/ Delivering_better_oral_health.pdf 2. .
8 Sheiham A. IS THERE A SCIENTIFIC BASIS FOR SIX-MONTHLY DENTAL EXAMINATIONS? Lancet 1977. doi:10.1016/S0140-6736(77)90620-1.
9 American Academy of Pediatric Dentistry. Guideline on periodicity of examination, preventive dental services, anticipatory guidance/counseling, and oral treatment for infants, children, and adolescents. Pediatr. Dent. 2016; 38: 133–141.
10 Department of Health and Social Care (UK). Dental Contract Reform: Evaluation of the First Year of Prototyping 2016-2017. Available from assets.publishing.service.gov.uk/government/ uploads/system/uploads/attachment_data/file/709555/ evaluation-report-201. .
11 Steele J. NHS dental services in England – An independent review. Available from www.sigwales.org/wp-content/uploads/dh_101180.pdf. 2009. 2009.www.dh.gov.uk/publications.
12 National Institute for Health and Care Excellence (NICE). Dental Recall: Recall Interval between Routine Dental Examinations. NICE Clin Guidel 19 2004. doi:10.1039/j19690001101.
13 Oral Health Assessment and Review: Dental Clinical Guidance. Scottish Dental Clinical Effectiveness Programme (2011). .
14 Fee PA, Riley P, Worthington HV, Clarkson JE, Boyers D, Beirne PV. Recall intervals for oral health in primary care patients. Cochrane database Syst Rev 2020; 10. doi:10.1002/14651858.CD004346.pub5.
15 Clarkson JE, Pitts NB, Bonetti D et al. INTERVAL (investigation of NICE technologies for enabling risk-variable-adjusted-length) dental recalls trial: a multicentre randomised controlled trial investigating the best dental recall interval for optimum, cost-effective maintenance of oral health i. BMC Oral Health 2018; 18: 135.
16 Conway DI, Purkayastha M, Chestnutt IG. The changing epidemiology of oral cancer: Definitions, trends, and risk factors. Br Dent J 2018; 225: 867.
17 Purkayastha M, McMahon AD, Gibson J, Conway DI. Is detecting oral cancer in general dental practices a realistic expectation? A population-based study using population linked data in Scotland. Br Dent J 2018; 225: 241–246.
18 UK National Screening Committee. Criteria for appraising the viability, effectiveness and appropriateness of a screening programme. 2015. Available at: https:// www.gov.uk/government/publications/evidencereview-criteria-national-screening-programmes/ crit. .
19 Watt RG. COVID-19 is an opportunity for reform in dentistry. Lancet 2020; 396: 462.
20 Information Services Division and NSS Practitioner Services on behalf of the Scottish Dental Practice Board. Primary Care Dentistry in Scotland Annual Report 2018/19. www.isdscotland.org/Health-Topics/Dental-Care/General. .
Comments are closed here.