BDA Scotland launches oral cancer action plan
Diagnosing oral cancer in practice is not at all easy, and incidences are increasing at a faster rate than any other cancer. The BDA’s latest report underscores the need for urgent and far-reaching changes to tackle the issue, but it does not hold all the answers
THE figures around oral cancer in Scotland make for sobering reading. It now kills more than three times as many people in Scotland as car accidents, and it’s on the increase. In November, the BDA Scotland launched Oral Cancer: A plan for action, a report which lays out its recommendations for tackling this growing issue, focusing on three key areas: prevention; early detection; and joined-up services.
There is no doubt that oral cancer needs significant focus, and the BDA report has done much to raise awareness in the media and, hopefully, with politicians that oral cancer is a growing problem and one that cannot simply be ignored or dealt with through simple public health initiatives.
Tackling this requires real investment in infrastructure and resources, major cultural changes and a willingness by the Scottish Government and others to listen to the dental profession and finally accept that, in the words of Robert Donald, BDA Scotland Chair, dentists “are not tooth-smiths, we are oral physicians”.
Prevention
The BDA action plan calls for sufficient resources to be available for effective smoking cessation and alcohol treatment services. This is critical, as alcohol and tobacco are two of the three biggest causes of oral cancer.
This also fits with the government’s overarching public health objectives in these areas. It is hoped that the introduction of minimum pricing will go some way to help, and the recent announcement that the Scottish Government plans to consult on restricting the marketing of alcohol products has been welcomed, but this by itself may not be enough.
Certainly, the significant cuts to smoking cessation services in Scotland over recent years seem to fly in the face of this objective, and we must hope that more resources are made available.
The third major cause of oral cancer is, of course, the HPV virus. The Scottish Government has indeed led the way in introducing the HPV vaccine for boys, and this development, which has followed years of campaigning, is to be applauded. There is now significant pressure from the same campaigners, including the BDA, to implement the programme of vaccinations as soon as possible, and, critically, to introduce a catch-up programme for older children who are still at school.
Speaking at the launch of the action plan, Minister for Public Health, Sport and Wellbeing, Joe Fitzpatrick, was unable to give a date for the implementation of the programme and would not commit to a catch-up programme. It is to be hoped that more concrete plans about the initial programme, and a commitment to the catch-up programme will be announced soon.
“Tackling this requires a willingness by the Scottish Government and others to listen to the dental profession”
Early detection
There is absolutely no doubt that early detection is critical. The BDA’s action plan calls for approaches to target those individuals who “do not engage regularly with oral health services”, as well as raising awareness of the early signs of suspected oral cancer to encourage dental visits. Both, laudable and important actions.
However, changing the behaviour and understanding of individuals requires significant, sustained and ongoing investment in major education and engagement programmes. It also requires wholesale change to how people view their interactions with the dental profession and access to dental services.
The Scottish Government response to this, and the BDA’s ongoing concerns about the plan for 24-month recall intervals, was to highlight the new personalised care plans described in the OHIP, as well as to emphasise the importance of self-examination.
There is still a lack of clarity about the mechanics around the new care plans and the resources needed to carry out oral health risk assessments for every patient. Self-examination for oral cancer is fraught with difficulty, which is not to say that the public should not have awareness of warning signs and be educated to look out for them, but relying on self-examination to fill the gap in between longer dental appointments could be considered short-sighted at best.
There is the argument that 24-month recall will only apply to low-risk patients, but if there is one thing that we can be sure of, it is that cancer does not discriminate, and low-risk does not mean no risk. However, the ongoing disagreement around recall intervals is complicated, with competing data on both sides of the argument, and should not be allowed to overshadow other elements required to tackle oral cancer.
Joined-up services
The BDA action plan calls for the simplification and streamlining of current referral processes to create one referral process for oral cancer across Scotland, citing the Glasgow Referral Pathway and Timeline as current best practice, while allowing that there is still room for improvement in it. There is no doubt that the current mixture of referral pathways
is untenable, but there remain questions as to why the Glasgow Pathway has been recommended.
It will be important to thoroughly analyse pathway requirements, consult more widely among the surgical teams and oncologists dealing with oral cancer, and investigate, for example, why the current UCS (Urgent Cancer Suspected) pathway on SCI Gateway, which is used for all other cancers, could not work for oral cancer. This is the referral pathway currently used by GPs who have urgent suspected oral cancer cases, and it is also already available to GDPs. It is also important to remember when considering this that oral medicine as a specialty is only available in tertiary centres, and any referral pathway must work everywhere.
It will also be important to tackle the elephant in the room. Many GDPs will refer for second opinion because they have a genuine fear of action from the GDC, should they make a mistake.
In summary, the BDA’s plan for action is an important first step in tackling the growth of oral cancer. To really move forward, however, will require the further involvement of, and consultation with, the dental profession, as well as major investment and commitment from the Scottish Government, the NHS and other stakeholder organisations.
Tackling oral cancer is complicated and multi-factorial, but there is much that can be done with the will, the investment and the commitment of everyone.

Do you know which of these is cancer?


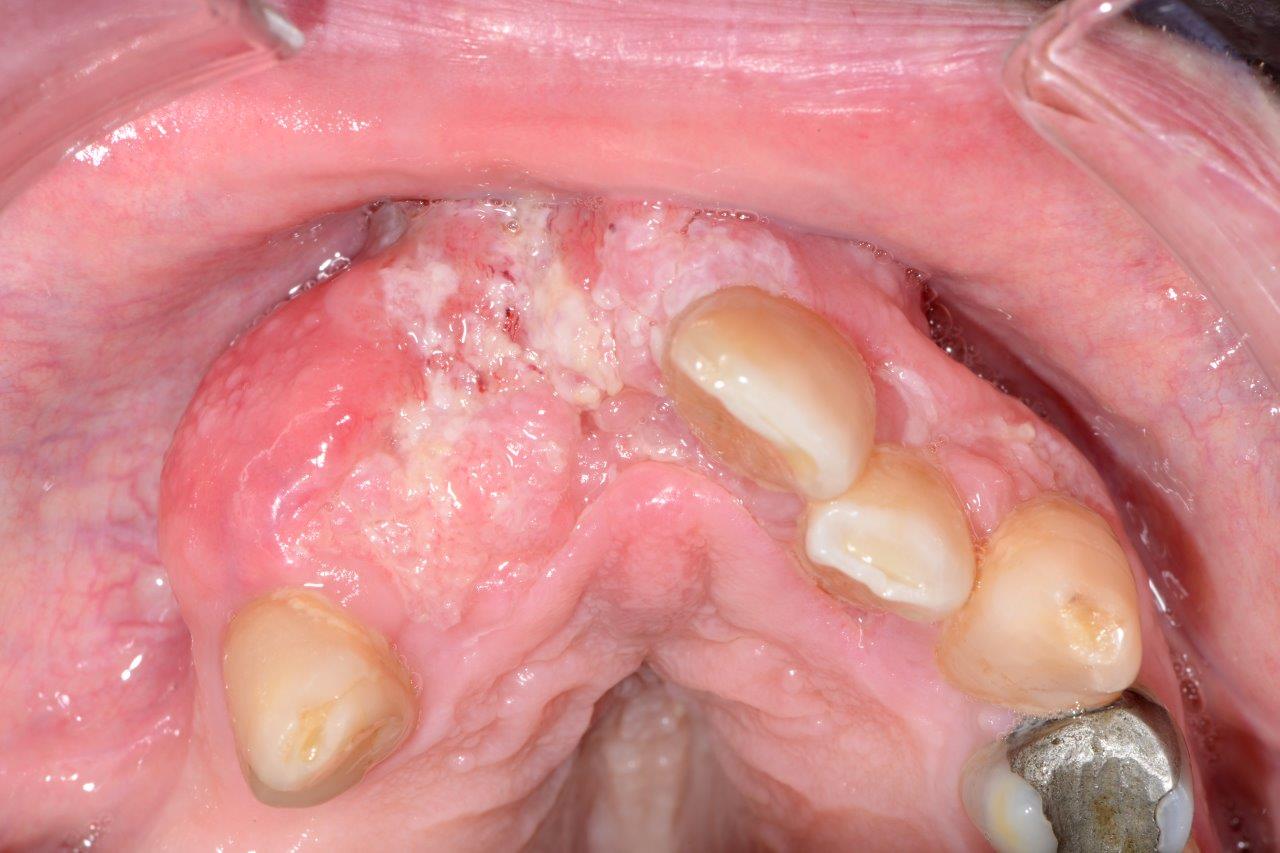


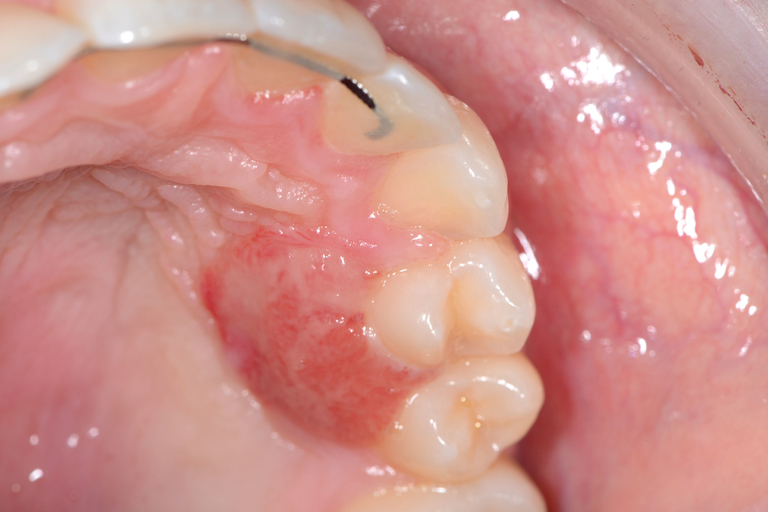


Even for experienced professionals, never mind the patients, recognising and diagnosing oral cancer is notoriously difficult.
At our Scottish Dental Show earlier this year, the audience at a lecture on oral cancer recognition and referral was shown these clinical slides of various oral cancer signs. The lecturer asked them to say which they would refer as high risk, an exercise, as it turned out, that proved very difficult for participants.
Slides that everyone agreed could only be malignant proved to be benign, and slides which showed cases that looked innocuous were quite the opposite. So, can you identify these conditions? (Answers below)
The answers: 1 – denture stomatitis, Benign; 2 – early tongue cancer; 3, large alveolar cancer; 4, large drug-related ulcer, benign; 5, lichenoid reaction with fungal infection, benign; 6, peripheral giant cell granuloma, benign; 7, retromolar cancer; 8, small floor of mouth cancer.
Comments are closed here.