
Reverse evidence-based dentistry bridging clinical reality and scientific evidence

The reality of modern clinical decision-making
Every practising dentist recognises the complexity of modern clinical decision-making: balancing professional judgement, patient expectations, rapidly evolving technologies and an ever-expanding body of scientific evidence; all within the practical constraints of time, workload, service pressures and real-world care.
In Scotland, where dentistry continues to evolve through prevention-focused models, quality improvement, reflective professional development and increasing digital integration, clinicians are navigating new layers of complexity; from artificial intelligence and digital diagnostics to shifting patient behaviours, widening health inequalities and growing recognition of oral–systemic health connections.
Evidence-Based Dentistry (EBD) remains the gold standard for informed clinical care. Yet in everyday practice, decisions rarely begin with a systematic review or formal guideline consultation. More often, they begin with something immediate and familiar; a recurring chairside observation, a clinical pattern that raises questions, or a treatment approach that appears to deliver meaningful outcomes. It is precisely at that point that Reverse Evidence-Based Dentistry begins.
rEBD was conceived as a way to bridge the gap between everyday practice and scientific inquiry, creating a more dynamic dialogue between observation and evidence
What Is Reverse Evidence-Based Dentistry?
Reverse Evidence-Based Dentistry (rEBD) is not a rejection of conventional EBD, nor an alternative to rigorous scientific appraisal. Rather, it is a complementary framework that begins where many clinical decisions begin, with observation in practice. A recurring treatment outcome, a pattern repeatedly seen in patients or a clinical approach that appears consistently effective may all prompt a simple but important professional question: “Why does this work, and what evidence truly supports it?”1
From that point, rEBD follows a structured pathway: clinical observation → focused question → targeted evidence search → critical appraisal → guideline alignment → refined clinical practice — moving backward from lived clinical experience toward scientific validation before returning forward into improved patient care.
Originally described as an educational and translational framework for strengthening reflective clinical reasoning, rEBD was conceived as a way to bridge the gap between everyday practice and scientific inquiry, creating a more dynamic dialogue between observation and evidence.¹,³ Properly understood, rEBD does not weaken EBD; it may, in fact, deepen it.
A conceptual framework of rEBD which transforms clinical observation into structured inquiry, scientific validation,
and refined patient care through an iterative cycle of evidence-informed practice. Adapted from Mascolo et al.¹
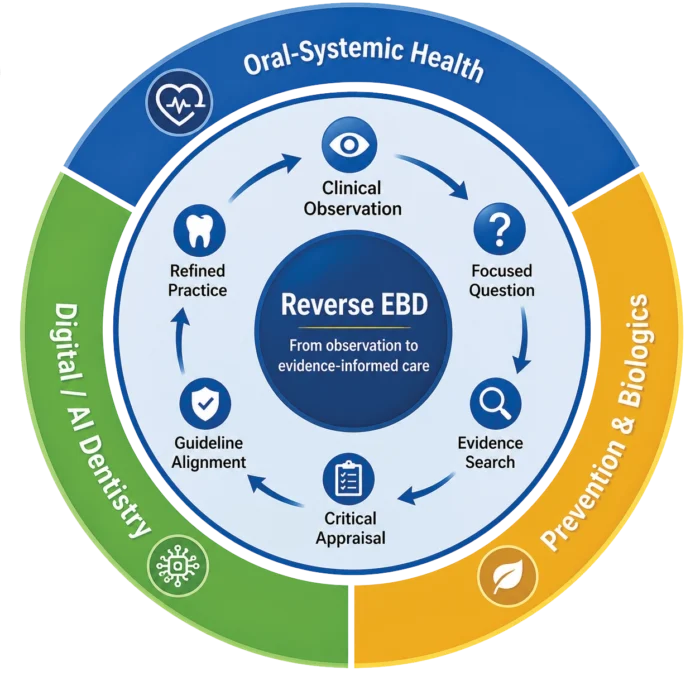
A conceptual framework of rEBD which transforms clinical observation into structured inquiry, scientific validation, and refined patient care through an iterative cycle of evidence-informed practice. Adapted from Mascolo et al.¹
Why this matters in Scotland now
Scotland provides a particularly relevant environment in which to consider the practical value of rEBD. The country combines a strong tradition of evidence-informed clinical guidance with growing emphasis on prevention, reflective professional development, quality improvement and service redesign.
At the same time, Scottish dentistry continues to navigate challenges familiar across modern healthcare systems: oral health inequalities linked to deprivation, variation in access between urban and rural communities, changing attendance patterns and increasing expectations placed on the wider dental team.5,6
These pressures are unfolding alongside rapid digital transformation, expanding discussion around skill mix and direct access models, and renewed focus on professionally reflective care pathways. Within this evolving landscape, clinicians are increasingly required not only to apply evidence, but to interpret it critically within the realities of everyday practice.
That is precisely where rEBD offers practical value. By encouraging clinicians to start from recurring chairside observations, formulate structured questions and reconnect practice with scientific appraisal, rEBD aligns naturally with Scotland’s culture of clinical audit, continuing professional development and evidence-informed service improvement. In this context, it is not simply a conceptual framework, it is a practical tool for modern Scottish dentistry.
Three chairside situations where rEBD makes a difference
rEBD becomes most valuable when applied to questions clinicians already encounter in everyday practice; not abstract theoretical problems but recurring chairside observations that deserve closer scientific attention.
Periodontal inflammation beyond the mouth
One example is the growing recognition that periodontal inflammation may extend beyond local oral tissues and interact with broader systemic pathways. Increasing evidence has linked periodontal inflammatory burden with markers of systemic inflammation, glycaemic control and cardiovascular risk profiles, encouraging a more integrated view of oral health within general healthcare.2 For clinicians, this changes the conversation: periodontal assessment is no longer only about pocket depth or bleeding scores, but potentially about quantifying inflammatory burden in ways that improve interdisciplinary communication, patient motivation, and preventive care planning.
rEBD begins with a familiar clinical observation and asks the next scientific question: how can we measure and communicate this relationship more meaningfully?
Artificial intelligence and clinical reasoning
A second example concerns the rapid integration of artificial intelligence into dentistry. From radiographic interpretation and digital planning to workflow automation and decision-support tools, AI is increasingly shaping clinical environments. Yet adoption itself is not evidence of benefit. Emerging educational and translational experience suggests that AI-assisted interpretation may influence clinical judgement, enhance diagnostic confidence and support less experienced clinicians — while also highlighting the well-recognised risk of automation bias.7
rEBD offers a practical filter here: not simply should we use AI, but how does AI influence our judgement and under what conditions does it genuinely improve care?
Prevention, biologics and minimally invasive care
A third area lies in preventive and biologically supportive dentistry. Whether considering bioactive agents, remineralisation strategies, low-intervention protocols, naturally derived therapeutic compounds or evolving implant biomaterials and surface technologies, clinicians are increasingly confronted with approaches that appear promising in practice before their mechanisms are fully understood.
Emerging evidence on biologically active materials – including antimicrobial natural compounds such as honey-derived systems – together with ongoing investigation into implant macro-morphology and surface characteristics, illustrates how long-observed clinical effects can stimulate new scientific questions when approached critically.8,9 In this way, rEBD reminds us that innovation is not always entirely new; sometimes it is familiar practice finally understood through stronger evidence.
From reflection to research: Scotland’s opportunity
Scotland is particularly well positioned to translate the principles of rEBD into meaningful clinical and professional progress. Few healthcare systems combine such a strong culture of evidence-informed guidance, reflective professional development, structured clinical audit and practice-based research. Through the work of the Scottish Dental Clinical Effectiveness Programme, continuing professional development frameworks supported by the General Dental Council and collaborative research initiatives across primary care, Scottish dentistry already possesses many of the foundations that rEBD requires; clinicians who observe critically, question constructively and continuously refine care through evidence and reflection.5,6
A practical next step may be surprisingly simple; transforming recurring chairside observations into structured clinical questions capable of generating meaningful evidence. Whether investigating periodontal inflammatory burden, evaluating AI-assisted diagnostic workflows or refining prevention-focused care pathways, Scottish clinicians are exceptionally well placed to contribute directly to the next generation of evidence-informed dentistry. In this sense, rEBD is not merely a conceptual framework; it is a practical bridge between everyday clinical observation and purposeful research.
Dentistry 5.0: why rEBD fits the future
Dentistry is entering a new era, increasingly shaped by artificial intelligence, digital workflows, bioengineering, personalised prevention and translational science. Yet innovation alone does not automatically translate into better care. New technologies may be adopted prematurely, interpreted uncritically or integrated without sufficient understanding of their true clinical value in everyday practice.3,7
This is precisely where rEBD becomes especially valuable. It functions as an analytical filter; a disciplined way of asking not simply: ‘What is new?’, but rather: ‘What is genuinely useful, for whom, and under what clinical circumstances?’
By linking innovation to clinical observation, scientific validation and reflective implementation, rEBD aligns naturally with the broader vision of Dentistry 5.0; a future in which technology supports professional judgement, strengthens patient-centred care and enhances clinical reasoning rather than replacing it.
One question every clinician can ask tomorrow
rEBD does not ask clinicians to move away from evidence, it invites them to engage with it more actively, beginning from the realities of everyday clinical care. Meaningful research questions do not always emerge from laboratories, policy papers or conference stages; often, they begin quietly at chairside, in the repeated observations that shape professional judgement over time.
A practical challenge for the months ahead is simple; choose one recurring clinical decision in your daily work – whether related to periodontal care, prevention, referral pathways or digital technologies – and ask: What evidence truly supports this approach in my patients, in my practice and in my clinical setting? That is not merely a reflective question; it is where Reverse Evidence-Based Dentistry begins.
Clinical vignette: Reverse EBD in everyday practice
A familiar chairside challenge
A 52-year-old patient presents repeatedly with signs of peri-implant mucositis; bleeding on probing, localised inflammation and intermittent discomfort around a posterior implant restoration. Oral hygiene appears satisfactory, plaque accumulation is limited and the prosthetic design is accessible for cleaning. Conventional advice has been reinforced, professional maintenance provided
and yet inflammation continues to recur.
At this point, rEBD asks a different kind of question.
- Rather than assuming inadequate plaque control is the sole explanation, the clinician pauses to explore broader possibilities:
- Is biofilm quantity truly the main driver, or is biofilm composition more relevant?
- Could host inflammatory burden or systemic low-grade inflammation be amplifying the local response?
- Do implant surface characteristics, emergence profile, or prosthetic contours contribute to plaque retention or altered tissue interaction?
- What does current evidence suggest regarding adjunctive therapies, local antimicrobials, or biologically active agents?
- Are there patient-specific behavioural, metabolic, or immunological factors that standard maintenance protocols fail to address?
What began as a recurring clinical observation is transformed into a focused scientific inquiry.
The clinician moves from “Why is this happening again?” to “What evidence can better explain what I am observing?”
This is rEBD in practice: observation → structured question→ targeted evidence search→ refined patient-centred management
In this way, chairside frustration becomes an opportunity for deeper understanding — and ultimately, better care.
About the author
Andrea Mascolo is Academic Director, European Institute for Medical Studies (EIMS), Malta and Full Professor of Digital Dentistry and Innovative Clinical Training, Grigol Robakidze University, Georgia.
Selected references
- Mascolo A, Dinculescu O, Mezetti M, Mercieca G, Busuttil F. Reverse Evidence-Based Dentistry: an innovative approach to dental education and clinical practice. Cureus. 2025;17(10):e94156. doi:10.7759/cureus.94156.
- Mascolo A, Dinculescu O, Bassignani J, Bensaidi S. Quantifying periodontal inflammatory burden: a conceptual clinical framework integrating periodontal inflamed surface area (PISA) and high-sensitivity C-reactive protein (hs-CRP) for oral-systemic health. Cureus. 2026;18(4):e106798. doi:10.7759/cureus.106798.
- Mascolo A, Bugelli G, Dinculescu O, Kipper MJ, Baghersad S. Dentistry 5.0: an emerging framework integrating bioengineering, artificial intelligence, and global innovation pathways for equitable oral health. Cureus. 2026;18(1):e102000. doi:10.7759/cureus.102000.
- Sackett DL, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71-72. doi:10.1136/bmj.312.7023.71.
- Public Health Scotland. NHS Dental Statistics for Scotland. Edinburgh, Scotland: Public Health Scotland; latest report.
- General Dental Council. Enhanced CPD Guidance for Dental Professionals. London, UK: General Dental Council.
- Khera R, Simon MA, Ross JS. Automation bias and assistive AI: risk of harm from AI-driven clinical decision support. JAMA. 2023;330(23):2255-2257. doi:10.1001/jama.2023.21082.
- Valente F, et al. The role of honey in dental caries prevention: a narrative review. Cureus. 2026;18(4):e106948. doi:10.7759/cureus.106948.
- Valente P, Sbrenna L, Mascolo A, et al. Dental implant macro-morphology and surface characteristics: a narrative review. Cureus. 2026;18(4):e106541. doi:10.7759/c.
Comments are closed here.