
The establishment of atraumatic tooth extraction
Performing atraumatic tooth extraction using piezoelectric surgery simplifies the procedure and yields superior outcomes compared with conventional methods, writes Dr José Carlos Rosas Díaz
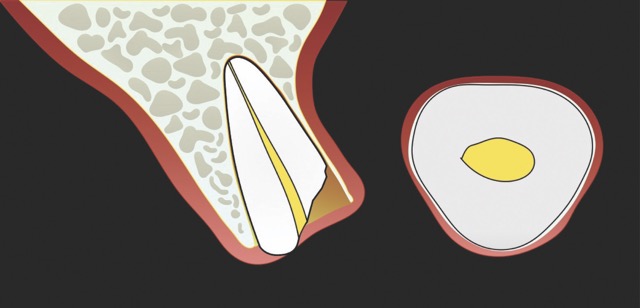
Figure 1: Single-rooted tooth remnant with extensive coronal destruction and a subcrestal fracture
Tooth extraction is a surgical procedure routinely performed by most dental practitioners. However, with the emergence of dental implants, meticulous management of both hard and soft tissues during the extraction has become increasingly evident. 1 2
Post-extraction, significant dimensional changes occur in the remaining structures due to horizontal and vertical crestal bone resorption. These changes coincide with the progressive replacement of the empty socket by granulation tissue, connective tissue, provisional bone, and eventually, mature lamellar bone. 2 3
Atraumatic tooth extraction facilitates the preservation of both soft and hard tissues, promotes an enhanced biological response for bone formation, and establishes a more favourable environment for immediate implant placement or alveolar ridge preservation.
This technique is particularly well-suited for patients with a thin gingival biotype, where it helps to prevent aesthetic complications
Post-extraction horizontal bone loss affects approximately 30% of the buccal plate and 10% of the lingual plate.³ Studies indicate that up to 50% of the buccal plate may be lost within the first year.4 These dimensional changes correspond to reductions ranging from 2.6 mm to 4.5 mm in width and from 0.4 mm to 3.9 mm in height at the crestal level.5
Pre-existing conditions, such as thin buccal bone plates (< 1 mm), can further exacerbate this situation leading to post-extraction bone loss of up to 1.17 mm in height and 2.67 mm in width. Conversely, thick buccal plates (> than 1 mm) exhibit significantly less resorption, with losses of approximately 0.5 mm in height and 1.17 mm in width.6 Additionally, greater crestal resorption has been reported following multiple extractions compared to single-tooth extractions.5
Atraumatic tooth extraction refers to the meticulous removal of the tooth, aimed at minimising iatrogenic trauma commonly associated with conventional extraction methods. This approach preserves both soft and hard tissues, fostering an enhanced biological response for bone formation and socket filling, mitigating the risk of postoperative infection, maintaining the natural gingival tissue contour, improving the aesthetic outcome of the final restoration, and providing a more favourable environment for immediate implant placement or alveolar ridge preservation.7











Whenever feasible, atraumatic tooth extractions are conducted via flapless techniques, thereby fostering optimal bone regeneration by preventing soft tissue invagination and reducing postoperative gingival recession. Flapless surgical approaches were introduced due to their potential biological advantages, such as accelerated healing and, most importantly, the reduction of bone resorption associated with the loss of gingival perfusion when soft tissues are detached from the underlying bone.8 This technique is particularly well-suited for patients with a thin gingival biotype, where it helps to prevent aesthetic complications.9
Numerous consensus reports agree that the integrity of the buccal bone plate is the key determinant for a favourable aesthetic outcome, particularly in the anterior region.7,10-12
Traditional extraction techniques remove the tooth utilising rotational movements and strong traction, thereby tearing Sharpey’s fibres from the bundle bone. This aggressive disruption of the periodontal ligament and associated fibres results in uncontrolled trauma within the alveolar socket, leading to a more pronounced collapse of the vascular network and subsequent resorption in the affected area.13
In contrast, the atraumatic piezoelectric technique allows precise positioning of instruments at the gingival sulcus level. These instruments advance between the root surface and the alveolar socket walls to a depth of up to 10 mm, facilitating the selective severing of only the most apical fibres. This approach enables gentle extraction and preservation of the crestal area, thereby significantly reducing the risk of bone resorption.14
Beyond its well-documented advantages in generating clean and precise cuts, piezoelectric surgery enhances the operator’s visibility, particularly when working in proximity to critical anatomical structures (e.g. vascular or neural bundles) and/or adjacent teeth exhibiting compromised proximal bone.15This improved control helps to prevent iatrogenic complications.16,17 Furthermore, the technique requires minimal applied pressure thereby reducing heat generation at the surgical site. 18
Bone removal around the tooth is characterised by its minimal and multidirectional nature, a distinct advantage over conventional techniques, which apply variable and unidirectional forces.11
When planning an atraumatic extraction, it is essential to consider key anatomical criteria such as root length, number of roots, and complex root morphology, as well as the presence of coronal remnants, previous endodontic treatment, or ankylosis. In such cases, it is important to highlight that piezoelectric devices offer a wide range of insert designs, which can be selected to match the specific morphology and spatial configuration of the root structure.14
Clinical Applications
Upon completion of atraumatic tooth extraction, either alveolar ridge preservation or immediate implant placement with concomitant regeneration will be performed, as indicated by the individual case.
Clinical case
A 68-year-old male patient presented with mobility of teeth 1.1, 2.1, and 2.2 after localised trauma. Clinical examination revealed root fractures and implant-supported restorations on adjacent teeth. Cone-beam computed tomography (CBCT) confirmed the clinical findings pertaining to the incisors, and atraumatic extractions were consequently indicated. Based on the dimensions of the remaining apical and palatal bone structures, which afforded predictable primary stability, post-extraction dental implants were planned, accompanied by simultaneous bone regeneration.




















Conclusion
Atraumatic tooth extraction facilitated by piezoelectric surgery offers biological advantages, including accelerated healing and reduced bone resorption. This flapless protocol has gained considerable importance following the advent of dental implant therapy.
About the author

Dr José Carlos Rosas Díaz, former Director of the School of Stomatology at the Universidad Privada San Juan Bautista (UPSJB) in Lima, Peru, holds a Master’s degree in stomatology and serves as a researcher at the UPSJB. He is a specialist in Comprehensive Oral Rehabilitation, Comprehensive Oral Implantology, and Periodontology.
References
- Lui JN, Khin MM, Krishnaswamy G, et al. Prognostic factors relating to the outcome of endodontic microsurgery. J Endod. 2014;40(8):1071-1076.
- Kerekes K, Tronstad L. Long-term results of endodontic treatment performed with a standardized technique. J Endod. 1979;5(3):83-90.
- Lieblich SE. Endodontic surgery. Dent Clin North Am. 2012;56(1):121-ix.
- Walton RE, Ardjmand K. Histological evaluation of the presence of bacteria in induced periapical lesions in monkeys. J Endod.1992;18(5):216-27.
- Tronstad L, Barnett F, Cervone F. Periapical bacterial plaque in teeth with refractory to endodontic treatment. Endod Dent Traumatol. 1990;6(2):73-7.
- Jepsen K, Schneider E, Dommisch H, et al. Management of a Central Incisor with Horizontal Root Fracture for Esthetic and Functional Rehabilitation. Int J Periodontics Restorative Dent. 2016;36(1):65-73.
- Brito-Junior M, Faria-e-Silva AL, Quintino AC, et al. Orthograde retreatment failure with extruded MTA apical plug in a large periradicular lesion followed by surgical intervention: case report. Gen Dent. 2012;60(2):96-100.
- Szalma J, Soós B, Krajczár K, et al. Piezosurgical management of sealer extrusion-associated mental nerve anaesthesia: A case report. Aust Endod J. 2019;45(2):274-280.
- Kang M, In Jung H, Song M, et al. Outcome of nonsurgical retreatment and endodontic microsurgery: a meta-analysis. Clin Oral Investig. 2015;19(3):569-582.
- Abella F, de Ribot J, Doria G, et al. Applications of piezoelectric surgery in endodontic surgery: a literature review. J Endod. 2014;40(3):325-332.
- Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endod. 2006;32(7):601-23.
- Song M, Nam T, Shin SJ, Kim E. Comparison of clinical outcomes of endodontic microsurgery: 1 year versus long-term follow-up. J Endod. 2014;40(4):490-494.
- Lofthag-Hansen S, Huumonen S, Gröndahl K, et al. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(1): 114-9.
- Strbac GD, Schnappauf A, Giannis K, et al. Guided Modern Endodontic Surgery: A Novel Approach for Guided Osteotomy and Root Resection. J Endod. 2017;43(3):496-501.
- Moreno-Rabié C, Torres A, Lambrechts P, et al. Clinical applications, accuracy and limitations of guided endodontics: a systematic review. Int Endod J. 2020;53(2):214-231.
- Kocyigit ID, Atil F, Alp YE, et al. Piezosurgery versus conventional surgery in radicular cyst enucleation. J Craniofac Surg. 2012; 23(6):1805-8.
- Hirsch V, Kohli MR, Kim S. Apicoectomy of maxillary anterior teeth through a piezoelectric bony-window osteotomy: two case reports introducing a new technique to preserve cortical bone. Restor Dent Endod. 2016;41(4):310-315.
- Gagliani M, Taschieri S, Molinari R. Ultrasonic root-end preparation: influence of cutting angle on the apical seal. J Endod. 1998;24(11):726-30.
- Rubinstein RA, Kim S. Short-term observation of the results of endodontic surgery with the use of surgical operation microscope and Super-EBA as root end filling material. J Endod. 1999;25(1):43-8.
- Del Fabbro M, Tsesis I, Rosano G, et al. Scanning electron microscopic analysis of the integrity of the root-end surface after root-end management using piezoelectric device: a cadaveric study. J Endod. 2010;36(10):1693-7.
- Tsesis I, Rosen E, Taschieri S, et al. Outcomes of surgical endodontic treatment performed by a modern technique: an updated meta-analysis of the literature. J Endod. 2013;39(3):332-9.
- Bastien AV, Adnot J, Moizan H, et al. Secondary surgical decompression of the inferior alveolar nerve after overfilling of endodontic sealer into the mandibular canal: Case report and literature review. J Stomatol Oral Maxillofac Surg. 2017;118(6):389-392.
Atraumatic Tooth Extraction: clinical perspectives
Professor Dr José Carlos Rosas Díaz is an expert in oral rehabilitation, implantology and periodontology. Drawing on his extensive experience in both research and clinical practice, he focuses on the benefits of atraumatic tooth extraction. Here, he discusses the preservation of the vestibular bone wall, the feasibility of immediate implant placement and the role of piezo technology in modern clinical practice.
What advantages do you see in atraumatic tooth extraction?
Atraumatic extraction enables us to remove teeth without damaging the vestibular (buccal) bone wall. This structure is typically very thin – often less than 0.5 mm – and therefore particularly susceptible to damage. At the same time, the proximal bone crest is preserved, which is especially important in the anterior region, where it plays a crucial role in maintaining the aesthetics of the gingival papillae. In the context of immediate implant placement, this approach offers significant benefits: the complete architecture of both hard and soft tissues can be preserved, resulting in a much more natural appearance of the implant restoration. For patients, this translates to reduced surgical trauma, greater comfort, and less postoperative pain and swelling. Additionally, in cases of dry socket (Alveoliti sicca), specialised piezoelectric instruments can be used to gently refine the alveolar walls. This careful micro-roughening of the bone surface stimulates renewed bleeding, substantially reducing the risk of dry socket and supporting uncomplicated healing.
Can you name cases in which immediate implantation would be possible following a conventional tooth extraction?
For successful immediate implant placement, certain clinical prerequisites must be met. There should be a minimum of 5 mm of apical bone remaining, and sufficient stable residual bone around the alveolus must be present to securely anchor the implant. Larger infectious lesions must be absent. Equally important is a vestibular (buccal) bone wall with a thickness of more than 1 mm. This stability can generally only be achieved through atraumatic extraction.
In your opinion, how does W&H piezo technology support atraumatic tooth extraction?
W&H offers very fine instrument tips (editor’s note: e.g., EX1 & EX2) with a diameter of only 0.2 mm. These allow precise entry into the periodontal ligament space, enabling controlled luxation of the tooth. With appropriate clinical skill, this significantly simplifies the extraction procedure. In particular, piezoelectric technology facilitates rapid and efficient extractions of severely ankylosed teeth in older patients or teeth with long-standing endodontic treatment. The specialised instrument geometry also allows for precise odontosections. In this way, atraumatic extraction becomes a safe and predictable procedure.
The W&H Group is a global leader in the development and manufacture of medical technology products.
Comments are closed here.