
Taking supported steps into full arch rehabilitation
Dr Anthony James shares a recent full arch rehabilitation case, for which he sought mentorship and guidance from an experienced clinician as part of his professional development

Screenshot
Treating your first full arch case can be a daunting experience, as it presents many more challenges than single-unit or shorter implant-retained bridge cases. In these instances, it is invaluable to have an experienced clinician who can help with the many stages this type of treatment entails.
Mentoring for this case was provided by Dr Callum Graham. From the treatment planning and case assessment stage through to the surgical phase, having someone else there to offer reassurance and guidance was essential. It afforded the confidence needed to successfully approach many more similar cases once this one was complete.
Case presentation
The patient, a 78-year-old female, had previously been advised by another dentist that she was not suitable for full-arch implant treatment without complex surgical solutions such as zygomatic implants and extensive sinus lifts. This was due to poor bone availability.
While this had not been attractive to the patient at the time, she had become fed up with wearing a denture and was very keen to see if any other implant treatment was possible.
Assessment and treatment planning
A new CBCT scan was taken to reassess whether this was an appropriate case for full-arch rehabilitation using the latest techniques and technologies available today. The results were analysed and shared with the mentor to discuss options; the outcome was positive and it was decided to see if a guided surgical approach would be possible.
The initial intention was to use Chrome GuidedSMILE to carry out this treatment, as it has the advantage of giving the patient a reasonably comfortable set of teeth straight away. This technology is made available across the Clyde Munro group as part of their commitment to innovation. The scans and photos were sent to the lab (Quoris) for design of the initial digital treatment plan.





However, the returned plan was not ideal. It included a large amount of bone reduction which was of concern. After consulting the mentor, the author decided that a freehand surgical approach would be more appropriate, using a staged loading approach. This would allow the flexibility to adapt during the surgical phase in order to deliver the best outcome despite the complexity of the case.
This was all explained to the patient in detail. Although the patient was a little disappointed that this would require a lengthier treatment time, with a denture to be worn during the healing phase, she was very understanding and happy to proceed. Informed consent was recorded.
A plan was created digitally by the mentor and mentee in collaboration to provide a blueprint for the freehand surgery. This made clear the clinical sequence to be followed, from extractions to the placement of five implants. It also detailed the ideal implant positions to allow for the desired restorative outcome. The assessment revealed resorption of the alveolar ridge, which also indicated the potential need for bone augmentation.
Surgical intervention
The patient was booked in for the whole morning to allow absolute focus on the treatment to ensure everything went as smoothly as possible.
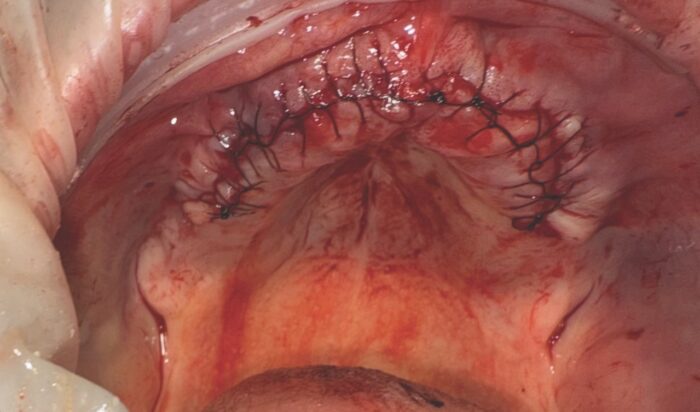
A full thickness flap was raised and the bone volume visually analysed. The alveolar ridge seemed in better shape than initially thought, so it was decided to place an additional implant in this region. Six implants were, therefore, placed, with the mentor helping to position the initial drill sites on the narrow ridge for optimal outcomes.
A bone graft was also required. For this, it was particularly useful to have the mentor in the room on the day of surgery. Dr Graham provided the equipment and expertise to facilitate the placement of a Puros Allograft blend. The patient’s blood was drawn, placed in the centrifuge and mixed with PRGF to create the membrane.
The site was then sutured closed, tension-free. The patient was given standard post-operative instructions to care for the surgical site and encourage uninterrupted healing.
A new provisional denture was provided as a temporary restoration. She returned to the practice after one week for review of the site and reported no issues. The final restoration will be provided after approximately six months of bone healing.
Debrief
The opportunity to discuss the above case with a mentor throughout the process, to have his support on the day and to debrief post-operatively was invaluable for me. I appreciate Dr Graham making himself readily available for any further help with this or any other cases in the future to help me deliver better outcomes for my patients as I progress in my implant surgery career.
Dr Graham was always easy to communicate with and he ensured a calm and reassuring environment for my first full arch surgery. With his clear advice and guidance, I never felt out of my depth or stressed.
About the author
Dr Anthony James has been practising in Edinburgh for more than 15 years and joined Gilmore Dental Practice in 2017. With a masters in aesthetic dentistry from King’s College London, he offers treatments including composite bonding, crowns, veneers, Invisalign and dental implants, catering to cases of all complexities. To offer the most advanced implant treatments for patients, he is currently enrolled in the prestigious European EAO Masters diploma programme.
The mentorship and guidance from an experienced clinician is part of Clyde Munro’s commitment to helping dentists advance in their careers.
Find out more about the career development opportunities available at Clyde Munro.
Comments are closed here.