
A rare intraoral presentation of lymphomatoid papulosis
McGrath G1, Bowen L2, Busuttil-Naudi K3, Forsyth C4, Wright S5
1Core Trainee in Oral Surgery & Special Care Dentistry, 2Core Trainee in Oral Surgery, 3Clinical Senior University Teacher/Honorary Consultant in Oral Surgery, 4Speciality Dentist in Oral Surgery, 5Consultant Pathologist
Department of Oral Surgery, Glasgow Dental Hospital & School, 378 Sauchiehall Street, Glasgow, G2 3JZ.
Department of Pathology, Queen Elizabeth University Hospital, 1345 Govan Road, Glasgow, G51 4TF.
Contact: grainnemcgrath39@outlook.com
Background
Lymphomatoid papulosis (LyP) is defined as a chronic, recurrent, self-healing papulonecrotic or papulonodular skin disease. (1)
- It is very rare, having an estimated incidence rate of 1.2-1.9 cases per million, with intraoral involvement even rarer with very few cases reported in the literature. (2)
- It displays a spectrum of histological appearances with its most concerning presentations suggestive of malignant lymphoma.
Despite its potentially alarming histology, the lesions tend to follow a benign clinical course resolving spontaneously within 3-12 weeks, sometimes leaving superficial scars. (1)
- It is characterised by recurrent crops of skin lesions, predominantly on the trunk and limbs.
- It tends to affect adults and can last for years or decades.
- It has no curative available treatment, but patients have a good prognosis with a 100 per cent five-year survival rate. (1)
Despite this, physicians tend to have a guarded approach as these patients have a small but increased risk of developing malignant lymphomas such as Hodgkins lymphoma or primary cutaneous anaplastic large-cell lymphoma. (1)
A case of intraoral LyP at Glasgow Dental Hospital is presented below, highlighting the challenges of diagnosing and managing this incredibly rare presentation.
Case description
A 72-year-old male was referred urgently by his consultant dermatologist to the Oral Surgery department at Glasgow Dental Hospital with regard to concerning tongue ulcers. He gave a four-day history of a tender and swollen tongue, which he associated with the onset of a new medication, sacubitril/ valsartan. The lesions arose two days after he started this medication. The sacubitril/valsartan was discontinued by the referring practitioner when he reported the tongue lesions. He had an extensive medical history including COPD, heart failure, myocardial infarctions and lymphomatoid papulosis affecting his skin, as well as polypharmacy. He was a heavy smoker and had a history of alcohol abuse.
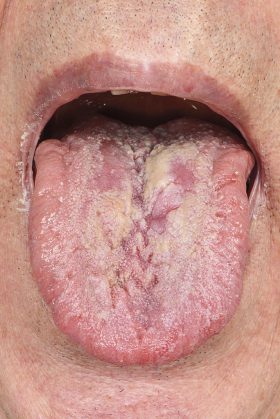
Extraoral examination was unremarkable. Intraoral examination revealed two large raised, firm ulcers on the left dorsal surface of the tongue crossing the midline. The larger ulcer measured 1.5cm in diameter. The acute onset of the lesions was unusual. Oral lesions are not listed as a side effect of sacubitril/valsartan in the BNF. Their concerning characteristics led to the provisional diagnosis of a squamous cell carcinoma and consequently an urgent incisional biopsy.
Histopathology
Histopathological analysis, from
the incisional biopsy of the tongue suggested a CD30 positive lymphoproliferative disorder.
Discussion
Without the availability of previous skin biopsies for comparison, a more sinister diagnosis may have been suspected, potentially leading to more aggressive and debilitating management.
The differential diagnosis included mucosal/cutaneous anaplastic T-cell lymphoma, mucosal/cutaneous involvement by systemic anaplastic lymphoma, transformed mycosis fungoides and lymphomatoid papulosis. Fortunately, identical cellular changes were seen in previous skin biopsies and the unusual and correct diagnosis of lymphomatoid papulosis of the tongue was given.
Oral involvement of LyP is incredibly rare, with fewer than 20 cases reported in the literature. (2) In these cases intraoral lesions predominantly affected the dorsal surface of the tongue, similar to this case, but lesions on the commissures and the uvula were also reported. For these cases, most of the patients already had a diagnosis of LyP affecting the skin prior to oral involvement, which would have greatly facilitated the diagnostic challenge.
The patient was under the care of Dermatology regarding his LyP skin lesions. Past management of his skin lesions included:
- a conservative approach – allowing time for spontaneous resolution
- excision
- topical steroids
Further treatment options suggested in the literature for LyP skin lesions include:
- a low-dose of oral methotrexate – the most effective treatment available to suppress the development of new LyP skin lesions
- PUVA (psoralen ultraviolet A light therapy)
- chemotherapy
Unfortunately, there is limited guidance in the literature on how to manage intraoral LyP lesions. However, as these lesions often resolve spontaneously, treatment is not always advocated.
After liaising with Dermatology, a topical betamethasone mouthwash was prescribed for symptomatic control and the lesions were monitored until they resolved within a three-week time period without incident.
Learning points
- Diagnosis and management of this rare condition and even rarer intraoral presentation proved challenging due to the lack of cases and guidance in the literature.
- As the condition can be easily misinterpreted for something more sinister, it is important that clinicians and pathologists are aware of this, to prevent unnecessarily aggressive management.
- Formal reporting of intraoral cases of LyP is crucial to build up a reference base for future clinicians.
- Long-term follow-up is important as these patients are at risk of developing a malignant lymphoma.
-

- Figure 1: Clinical photograph of the tongue ulceration at initial examination

-
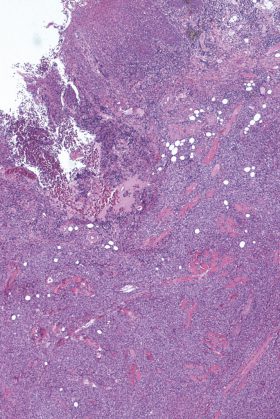
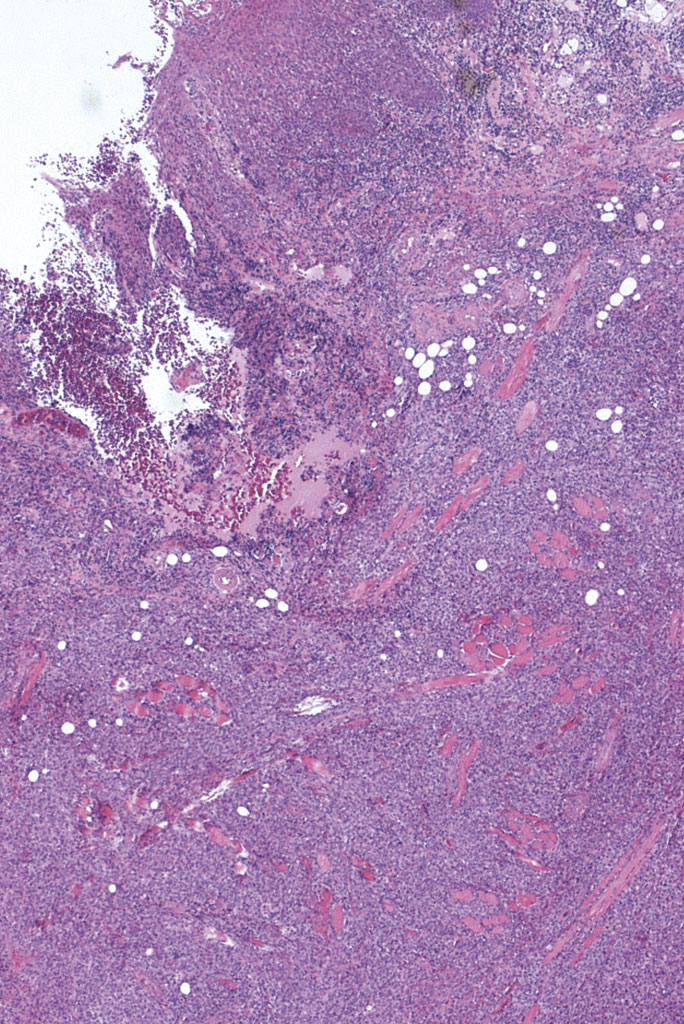
- Figure 2: Low-power view, X20 magnification, H&E stain It demonstrates: • heavily stratified squamous epithelium towards one edge • an area of ulceration towards the other edge • diffuse infiltrate of lymphoid cells in the underlying skeletal muscle bundles
-
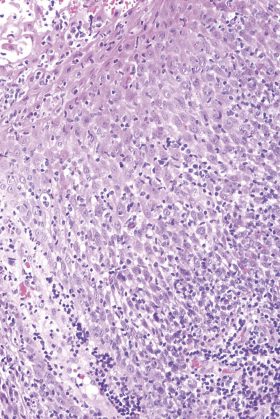
- Figure 3: Medium-power view, X100 magnification, H&E stain It demonstrates: • the squamous epithelium overlying the lymphoid infiltrate • there is no epidermotropism of the large lymphoid cells
-
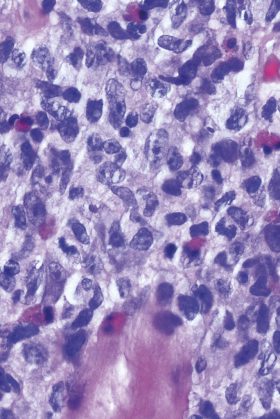
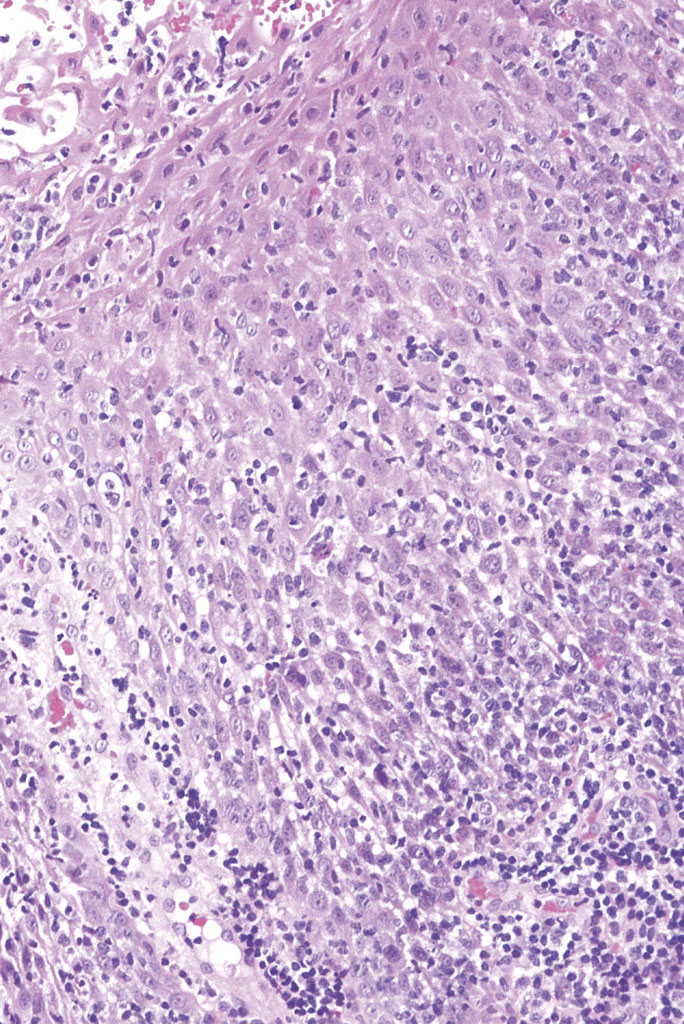
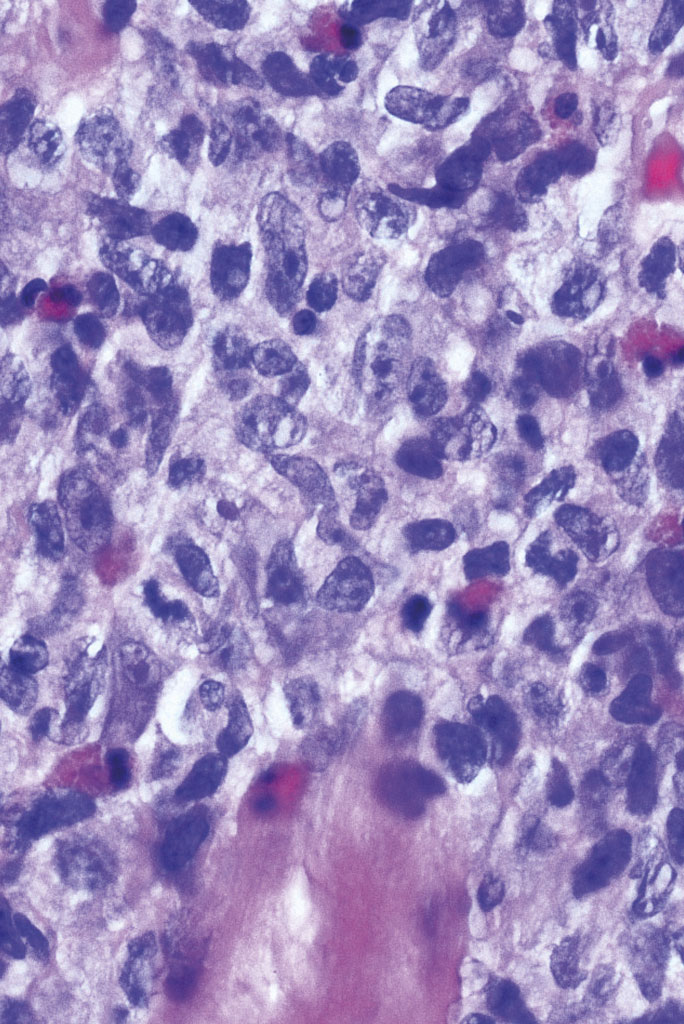
- Figure 4: High-power view, X400 magnification, H&E stain It demonstrates: • the lymphoid infiltrate • large, pleomorphic lymphoid cells with vesicular nuclei and prominent nucleoli
-
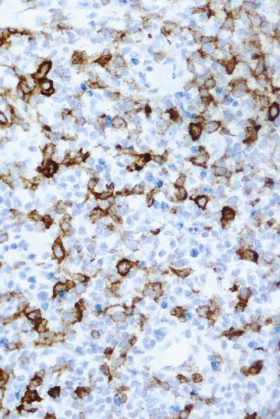
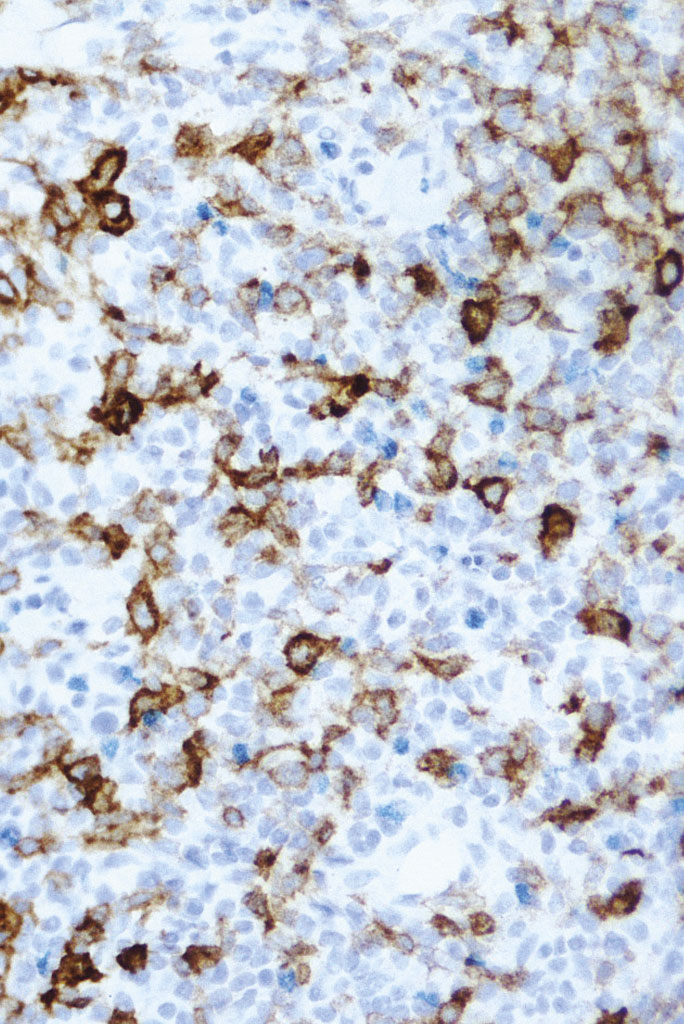
- Figure 5: High-power view, X200 magnification, CD30 immunostain It demonstrates: • the large lymphoid cells stained positively with CD30 immunostain in a membranous and cytoplasmic pattern
-
- Figure 6: Clinical photograph of the tongue at two-week review appointment. There was some firmness on palpation. The lesion had improved dramatically

References
1: Willemze R, Jaffe ES, et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005; 105:3768-3785
2: Sciubba J, Said-al-Naief et al. Critical review of lymphomatoid papulosis of the oral cavity with case report. Oral Surg Oral Med Oral Pathol Oral Endod 2000; 90:195-204
3: Belijaards RC, Willemze R. The prognosis of patients with lymphomatoid papulosis associated with malignant lymphomas. British Journal of Dermatology 1992; 126(6):596-602
4: Kempf W, Levi E, et al. Fascin expression in CD30-postive cutaneous lympoproliferative disorders. Journal of Cutaneous Pathology 2002. 29(5): 295-300
Comments are closed here.